Article Info
Year: 2023
Month: July
Issue: 3
Pages: 4-5
A cluster of confirmed Middle East respiratory syndrome (MERS) cases in Al-Hayat National Hospital (ANH) in Khames Mushait City reported by Asier Health Affairs (AHA) during January 2020. MERS is a fatal viral respiratory illness. More than half of the laboratory-confirmed MERS-CoV infections with a human-to-human transmission reported globally are healthcare-associated settings1.
On January 15, 2020, ANH Emergency Department (ER) received a patient complaining of shortness of breath (SOB) and fever. The patient is a Filipino female known to have Diabetes and Hypertension, works as a nurse in the outpatient department (OPD) at ANH, and was admitted as a severe pneumonia case. After three days, while the condition continued deterioration, PCR of the patient's nasopharyngeal (NP) swab for MERS-CoV tested positive. Then, two asymptomatic Healthcare Workers (HCWs) reported after contacts investigations. In addition to 3 cases reported from other hospitals are related to ANH outbreak. MERS patients were referred to a specialized hospital in Abha for proper isolation and treatment.
The Field Epidemiology Training Program team investigated the outbreak. The goals were to identify the infection source, transmission mode, follow-up the cases and contacts, and evaluate the hospital infection prevention and control (IPC) measures. The team reviewed the patients' medical records and MOH MERS forms in ANH and the specialized referral hospital, contacts investigation, follow-up lists, interviewed the staff and reviewed the IPC measures in the ER and OPD. As a case series study.
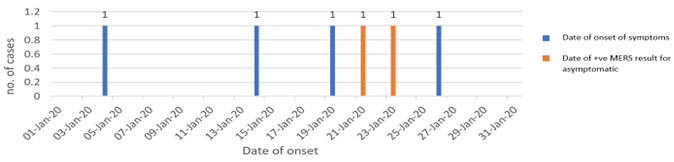
The team defined confirmed cases as any reported patient from AHA with laboratory-confirmed MERS-CoV infection from 19-1 to 29-1-2020. The probable case was defined as any reported patient from AHA who had clinical features and an epidemiologic link. The epidemiologic links were defined as the exposure to a confirmed case, contact with dromedary camels, or reported consumption of camel products, but with absent or inconclusive laboratory results for MERS-CoV infection during the same period2. The team identified a total of 6 confirmed MERS-CoV cases during the studied period. There were 66% female, 50% Saudi, 50% HCWs and 40% have chronic conditions (Asthma, Diabetes, and Hypertension). The mean age was 49 years (range: 28–72 years). Case Fatality Rate (CFR) 16%, Secondary attack rate (SAR) among HCWs was 0.86%, SAR among community contacts was 3.4%. Four cases (67%) reported symptoms (Figure1). They had respiratory symptoms, including cough, fever, and SOB. They sought medical assistance from various emergency departments. While the asymptomatic cases were discovered as part of the contacts investigation. The mean incubation period was 8 (range 4-11) days. All symptomatic and asymptomatic cases were hospitalized for isolation and close follow-up until NP swabs of MERS-CoV turned negative.
There were two probable cases; both were HCWs, provided care for the index case, and complained of fever, cough, and SOB. Both were tested for MERS-CoV three times due to the epidemiological links, but the NP swabs were negative.
ANH tested 228 HCWs contacts for MERS-CoV. AHA followed up 85 community contacts for the prolonged incubation period (14 days), only 21 showed symptoms and tested, where the results came negative.
Cases reported no history of direct or indirect contact with dromedary camels. all (HCWs) are trained on (IPC) measures.
Editorial notes: In 2012, MERS-CoV, first identified in the Middle East region. Saudi Arabia has the largest number of reported cases, with 2106 cases (19.1 % HCWs), 783 related deaths (CFR 37.2%), and the highest risk age group are 50-59 years old3. According to the team suggestion, the infection was introduced to the hospital by an undetected patient who had close contact with the index case. The delay in diagnosing the index case, the close contact of the secondary cases with the index case, along with the weak adherent of the HCWs to ICP measures and PPE using in the hospital words and clinics were responsible for spreading of the infection. Patients with severe complications were old age and had comorbidities. The symptomatic cases with –ve swab result may needed lower respiratory samples, which are more accurate4. According to the Saudi MERS guideline, there must be respiratory triage areas, and suspected/confirmed cases must be placed under isolation. Early detection of cases, adherence to IPC recommendations, and recognition of illness among HCWs are necessary factors to prevent transmission of MERS-CoV2.
Figure 1: Epidemic curve of confirmed MERS CoV cases in Khames Mushait, Saudi Arabi, Jan 2020.
References:
1. Middle East respiratory syndrome coronavirus (MERS-CoV) [Internet]. Who.int. 2019 [cited 11 February 2020]. Available from: https://www.who.int/news-room/q-a-detail/middle-east-respiratory-syndro…-(mers-cov)
2. MIDDLE EAST RESPIRATORY SYNDROME CORONAVIRUS; GUIDELINES FOR HEALTHCARE PROFESSIONALS [Internet]. 5th ed. Saudi Ministry of Health; 2018 [cited February 18 2020]. Available from: https://www.moh.gov.sa/CCC/healthp/regulations/Documents/MERS-CoV%20Gui…
3. WHO EMRO | MERS outbreaks | MERS-CoV | Health topics [Internet]. Emro.who.int. 2019 [cited 11 February 2020]. Available from: http://www.emro.who.int/health-topics/mers-cov/mers-outbreaks.html
4. Assiri A, Al-Tawfiq JA, Al-Rabeeah AA, Al-Rabiah FA, Al-Hajjar S, Al-Barrak A, Flemban H, Al-Nassir WN, Balkhy HH, Al-Hakeem RF, Makhdoom HQ. Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: a descriptive study. The Lancet infectious diseases. 2013 Sep 1;13(9):752-61.
Keywords: Middle East respiratory syndrome, coronavirus, MERS, Healthcare-associated outbreaks.
تقصي حالات فاشية فيروس متلازمة الشرق الاوسط التنفسية (كورونا) في مستشفى الحياة الوطني بخميس مشيط ,يناير ,2020م
الصحيه بعسير في مستشفى الحياة الوطني , بخميس مشيط 15 يناير 2020م , عندما أستقبل قسم الطوارئ بالمستشفى مريضة تشكو من ضيق في التنفس والحمى. تعمل المريضة كممرضة بعيادة الامراض الصدرية في نفس المستشفى ,فلبينية الجنسية,وتتعالج من أمراض السكر والضغط المزمنة. تم تنويمها كحالة التهاب رئوي. ظهرت نتيجة تحليل فيروس كورونا إيجابية بعد ثلاثة ايام (19يناير) مع استمرار تدهور حالتها الصحية . بعد ذلك تم الكشف عن بقية الحالات تباعا, حيث اكتشفت حالتين تعملان بالمستشفى و3 حالات لمرضى تواجدو بها,وتم الابلاغ عنهم من قبل مستشفيات أخرى, في الفترة من 19 وحتى 26 يناير . وقدعزلت جميع الحالات بمستشفى متخصص بعسير.
قام فريق من برنامج الوبائيات الحقلي بالتقصي في هذه الفاشية. وقد كان الهدف هو تحديد مصدرالعدوى,طريقة انتقالها ,متابعة الحالات ,تتبع المخالطين,وتقييم إجراءات الوقاية ومكافحة العدوى في المستشفى.
أجريت الدراسة الوصفية بمراجعة السجلات الطبية واستمارات تقصي وزارة الصحة للحالات والمخالطين , كما أجريت مقابلات مع المسؤلين بصحة عسير وموظفي المستشفى,وتم تقييم تدابير مكافحة العدوى.
تم تعريف الحالة المؤكده :أي مريض تم الابلاغ عنه من قبل صحة عسير مصاب بفيروس كورونا مؤكد مخبريا خلال الفترة من 19-29 يناير.الحالة المحتملة:أي مريض تم الابلاغ عنه من قبل صحة عسير ولديه أعراض وخطر وبائي (إتصال وثيق بالحالة المؤكده), مع عدم وجود نتائج مختبرية أو غير حاسمة لعدوى فيروس كورونا خلال هذه الفتره.
وجد مامجموعه 6 حالات إصابة بفيروس كورونا مؤكده خلال الفترة المذكورة . وكان منهم :66% إناث ,50% سعودين, 40% يعانون من أمراض مزمنه (السكر ,الضفط والربو).
بلغ متوسط أعمارهم 49عام(تراوحت من28-72عام). أربعة منهم عانو من أعراض الجهاز التنفسي.متوسط فترة حضانة المرض 8 أيام (تراوحت من 4-11 يوم).
كانت هناك حالتين إضافيتين محتملة قد عانت من أعراض الكورونا, ونظرا لإتصالهم الوثيق بحالة مؤكدة مخبريا تم عمل التحليل ثلاث مرات جميعها نتائجها سلبية.
228 عاملاً صحيا مخالطا بمعدل إصابة الثانوي (0.86٪) و85 مخالطا مجتمعيا بمعدل إصابة ثانوي (3.4٪).
لم يلاحظ أي تاريخ للأتصال المباشر وغيرالمباشر للأبل بين الحالات.
استنتج الفريق الذي قام بالقصي أن مصدر العدوى كان مريضا بدون أعراض ظاهره من خارج المستشفى اتصل بشكل مباشر مع الحاله الاولى. كما أدى ضعف تقيد العاملين الصحين في في المستشفى بتدابيرالوقاية و مكافحة العدوى إلى انتقال العدوى إلى العاملين الآخرين والمرضى عن طريق الاتصال المباشر.نتائج تحليل كورونا السلبيه لدى المرضى المحتملين ذوي نتائج تحاليل كورونا السلبيه قد يحتاجون الى أخذ مسحات من الرئتين مباشرة. بينما الأمراض المزمنه لدى أربع حالات أدت إلى دخولهم العناية المركزة ووفاة واحدة. لذلك ، يجب على المستشفى الالتزام بتطبيق إرشادات وزارة الصحة في الكشف عن حالات متلازمة الشرق الأوسط التنفسية وإدارتها جنبًا إلى جنب مع إجراءات الوقاية ومكافحة العدوى.
كلمات البحث: متلازمة الشرق الأوسط التنفسية ، فيروس كورونا ، متلازمة الشرق الأوسط التنفسية ، تفشي الأمراض المرتبطة بالرعاية الصحية.