Article Info
Year: 2025
Month: July
Issue: 3
Pages: 2-4
Globally, around four billion people, nearly half the world’s population, live in dengue-endemic areas, with an estimated 400 million infections each year, of which approximately 50-100 million become symptomatic [1].
Dengue fever caused by a Flavivirus transmitted predominantly by Aedes aegypti and Aedes albopictus mosquitoes, dengue virus is currently the most prevalent arboviral infection affecting humans worldwide [2]. By 2080, projections estimate that more than six billion individuals, nearly double the number at risk in 2015, could be susceptible to dengue virus infections, underscoring the urgency of enhanced control measures [1].
Though Saudi Arabia remained largely dengue-free until the mid-1990s, outbreaks have become increasingly frequent since 1994, marking the disease’s establishment as a significant public health challenge in the region [3,4]. By 2013, over 6,500 cases were reported, and more recent data from 2022 indicate 3,647 cases nationwide, including 115 cases in Riyadh [5].
Given Riyadh’s growing population, urban sprawl, and increased travel and migration, understanding the city’s dengue dynamics is critical. Our study aimed to fill the existing knowledge gap by identifying dengue virus high-risk demographic profiles in Riyadh region. In addition to analyzing seasonal and temporal patterns of dengue outbreaks and examining the association between recent travel history and dengue infection. Moreover, we assessed the knowledge and preventive practices among the reported cases in Riyadh region regarding dengue fever.
By achieving these objectives, our study will generate evidence-based recommendations to inform public health strategies for dengue prevention and control in Riyadh region, aligning with national priorities to combat vector-borne diseases.
We conducted a cross-sectional study using a secondary data of all dengue virus cases reported in Riyadh region, from Mid-September 2022 to December 2024. The dataset was obtained from the Ministry of Health, Vector-Borne Diseases Department. Our objectives were to assess dengue virus demographic characteristics in Riyadh region, identifying high-risk areas, analyzing the temporal trends and seasonal patterns of the disease and to investigate the relationship between some risk factors and dengue virus cases aiming to understand the epidemiology of dengue virus and its impact on public health in Riyadh region.
Out of 1544 recorded cases, 44.2% (N=683) were confirmed dengue cases. Among them, 85.2% were infected in 2023 and 2024. About 60% were aged between 25 - <45 years old, with the least infected age group being less than 15 years. Nearly two-thirds of cases were males, and almost half were Saudis. Majority of confirmed cases were located in Riyadh city (82.4%) and the most frequently reported neighborhoods of the cases were Alnarjis (10.5%) and Alaridh (7.5%). (Table 1)
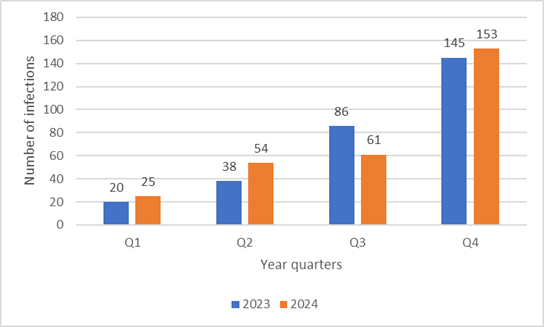
The quarterly distribution of confirmed dengue infections for both 2023 and 2024 reveals a consistent upward trend throughout each year, with a pronounced surge observed in the fourth quarter (October-December). In 2023, the number of cases rose steadily from 20 in Q1 (January-March) to 145 in Q4. Similarly, in 2024, infections increased from 25 in Q1 to 153 in Q4. Notably, the rise between Q3 (July-September) and Q4 was the most significant in both years (from 86 to 145 in 2023, and from 61 to 153 in 2024). (Figure 1)
Regarding factors associated with dengue virus infection, (Table 2) reveals that the mosquito exposure and presence of stagnant water are significantly different with Dengue infection (p-value 0.000, 0.003, respectively). The rate of exposure to mosquitoes was higher in the confirmed cases (50.8%, as compared to 35.4% in the probable cases), the rate of presence of stagnant water was relatively higher in the confirmed cases (25.5%, compared to 16.2% in the probable cases). Other factors, such as travel within 14 days, means and place of travel were insignificantly associated.
On assessing knowledge, the majority of the confirmed cases (89.9%) expressed that they know the risk factors that lead to mosquito proliferation. Factors related to water accumulation were the most mentioned (79.4%). The majority (85.8%) reported that they use mosquito repellent products. When confirmed cases were asked about diseases transmitted by mosquito bites, (43.8%) mentioned the dengue virus, (19.8%) mentioned malaria and (12.9%) mentioned both dengue and malaria.
Environmental factors significantly associated with infection included presence of stagnant water which create optimal breeding grounds for Aedes mosquitoes, whose flight range is limited [6]. The “Balady” platform by the Saudi government has improved public engagement by enabling community reporting of environmental hazards like stagnant water [7].
Our study showed many implications, highlighting significant dengue fever-related factors, trend of dengue fever cases, and displaying the seasonal variation, helping with better prevention in Saudi Arabia.
Our study highlights that adult males, especially non-Saudis living in northern Riyadh city, are most affected by dengue, particularly in the last quarter of the year. Key risk factors include mosquito exposure and stagnant water. Targeted dengue prevention efforts should focus on high-risk groups and intensifying vector control measures, particularly before and during the fourth quarter annually.
Table 1: Distribution of confirmed Dengue virus cases according to socio-demographic in Riyadh region, Saudi Arabia
| Variable | Categories | n=683 | |
| No. | % | ||
| Year of infection | 2022* | 101 | 14.8 |
| 2023 | 289 | 42.3 | |
| 2024 | 293 | 42.9 | |
| Age |
< 5 | 4 | 0.6 |
| 5-<15 | 22 | 3.2 | |
| 15-<25 | 61 | 8.9 | |
| 25-<35 | 203 | 29.7 | |
| 35-<45 | 203 | 29.7 | |
| 45-<55 | 88 | 12.9 | |
| 55-<65 | 63 | 9.2 | |
| >65 | 39 | 5.7 | |
| Age (Mean ± SD) | 38.6±14.8 | ||
| Gender | Male | 475 | 69.5 |
| Female | 208 | 30.5 | |
| Nationality | Saudi | 334 | 48.9 |
| Non-Saudi | 349 | 51.1 | |
| Geographic distribution | Riyadh city | 563 | 82.4 |
| Other Governorates in Riyadh | 8 | 1.2 | |
| Other regions in SA | 3 | 0.4 | |
| Unknown | 109 | 16 | |
| Neighborhood | Alnarjis | 72 | 10.5 |
| Alaridh | 51 | 7.5 | |
| Other** | 560 | 82 | |
|
SD= Standard Deviation SA= Saudi Arabia *= This almost represents Q4 of the year, since the detection of the first case in Riyadh region. **= None of the other neighborhoods is represented by a considerable proportion (i.e., < 5%), or even a considerable sample size (n < 25); thus, they were combined into "other" |
|||
Table 2: The quarterly distribution of confirmed dengue infections in Saudi Arabia for 2023 and 2024
| Variable | Category | Confirmed | Probable | p-value |
| No. (%) | No. (%) | |||
| Travel within 14 days | Yes | 89 (22.9%) | 103 (29.1%) | 0.065 |
| No | 299 (77.1%) | 251 (70.9%) | ||
| Means of travel | Plane | 53 (60.9%) | 65 (65%) | 0.314 |
| Car | 33 (37.9%) | 30 (30%) | ||
| Bus | 0 (0%) | 3 (3%) | ||
| Ship | 1 (1.1%) | 2 (2%) | ||
| Travel place | Within SA | 50 (57.5%) | 53 (52.5%) | 0.530 |
| Out of SA | 35 (40.2%) | 47 (46.5%) | ||
| Within and Out Of SA | 2 (2.3%) | 1 (1%) | ||
| Exposure to mosquitoes | Yes | 197 (50.8%) | 125 (35.4%) | 0.000* |
| No | 118 (30.4%) | 141 (39.9%) | ||
| Not sure | 73 (18.8%) | 87 (24.6%) | ||
| Presence of stagnant water | Yes | 98 (25.5%) | 57 (16.2%) | 0.003* |
| No | 287 (74.5%) | 294 (83.8%) | ||
|
SA= Saudi Arabia *= p-value is considered significant if <0.05 at a 95% confidence level |
||||
Figure 1: The quarterly distribution of confirmed dengue infections in Saudi Arabia for 2023 and 2024
Reference:
1. Messina JP, Brady OJ, Golding N, Kraemer MUG, Wint GRW, Ray SE, et al. The current and future global distribution and population at risk of dengue. Nat Microbiol. 2019;4:1508-15. doi: 10.1038/s41564-019-0476-8
2. Gubler DJ. Dengue, Urbanization and Globalization: The Unholy Trinity of the 21st Century. Trop Med Health. 2011;39:S3-S11. doi: 10.2149/tmh.2011-S05
3. Shepard DS, Undurraga EA, Halasa YA, Stanaway JD. The global economic burden of dengue: a systematic analysis. The Lancet Infect Dis. 2016;16:935-41. doi: https://doi.org/10.1016/S1473-3099(16)00146-8
4. Al-Tawfiq JA, Memish ZA. Dengue Hemorrhagic Fever Virus in Saudi Arabia: A Review. Vector-Borne and Zoonot Dis. 2018;18:75-81. doi: 10.1089/vbz.2017.2209
5. Saudi Ministry of Health. Statistical Yearbook [Internet]. 2022 [cited 2025 July 1]. Available from:https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistica….
6. Hoque MA-A, Sardar ML, Mukul SA, Pradhan B. Mapping dengue susceptibility in Dhaka city: a geospatial multi-criteria approach integrating environmental and demographic factors. Spat Inf Res. 2025;33:33. doi: 10.1007/s41324-025-00635-y
7. Balady Services. [Internet]. [cited 2025 Jul 1]. Available from: https://balady.gov.sa/en.
الوضع الوبائي لعدوى فيروس حمى الضنك في منطقة الرياض، المملكة العربية السعودية: دراسة مقطعية (سبتمبر 2022 - ديسمبر 2024)
يعيش حوالي أربع مليار شخص حول العالم أي ما يقارب نصف سكان الكرة الأرضية في مناطق موبوءة بحمى الضنك كما يتم تسجيل نحو 400 مليون إصابة سنويًا، منها ما بين 50 إلى 100 مليون حالة تظهر عليها الأعراض. تنتقل حمى الضنك بشكل رئيسي عن طريق البعوضة الزاعجة المصرية. تشير التقديرات إلى أنه بحلول عام 2080 قد يصبح أكثر من ست مليارات شخص معرضين للإصابة بحمى الضنك وهو ما يُقدر بضعف عدد المعرضين للإصابة في عام 2015 تقريبًا مما يعكس الحاجة الملحة لتعزيز التدابير الوقائية.
رغم أن المملكة العربية السعودية كانت شبه خالية من حمى الضنك حتى منتصف التسعينيات، إلا أن الفاشيات بدأت تظهر بوضوح منذ عام 1994 مما جعل المرض يمثل تحديًا صحيًا متزايدًا. أظهرت بيانات عام 2022 تسجيل 3,647 حالة على مستوى المملكة منها 115 حالة في منطقة الرياض.
نظرًا للنمو السكاني السريع والتوسع العمراني وازدياد السفر والهجرة لمدينة الرياض فإن فهم ديناميكية انتشار حمى الضنك في المدينة أصبح أمرًا بالغ الأهمية. تهدف هذه الدراسة إلى سد الفجوة المعرفية من خلال تحديد الفئات السكانية الأكثر عرضة للمرض وتحليل الأنماط الموسمية والزمنية لتفشي المرض ودراسة العلاقة بين تاريخ السفر والإصابة بالمرض، إضافة إلى تقييم مستوى المعرفة والممارسات الوقائية لدى الحالات المُبلّغ عنها.
أُجرينا دراسة مقطعية باستخدام بيانات ثانوية لجميع حالات فيروس حمى الضنك المُبلّغ عنها في منطقة الرياض في الفترة من منتصف سبتمبر 2022 وحتى ديسمبر 2024، وذلك بالاعتماد على سجلات الإدارة العامة لنواقل المرض بوزارة الصحة.
من بين 1544 حالة مسجلة، كانت هناك 683 حالة مؤكدة (44.2٪). شكلت الفئة العمرية ما بين 25 وأقل من 45 عامًا معظم الاصابات بينما كانت الفئة الأقل إصابة هي ما تحت سن 15 عامًا. شكل الذكور حوالي ثلثي الحالات وكان نحو نصف المصابين من الجنسية السعودية. سُجّلت 82.4٪ من الحالات المؤكدة داخل مدينة الرياض، وخاصة في أحياء النرجس (10.5٪) والعارض (7.5٪).
أظهرت بيانات دراستنا نمطًا متكررًا للزيادة الفصلية، وبلغت ذروة الإصابات في الربع الرابع (شهر أكتوبر – ديسمبر). في عام 2023 ارتفعت الحالات من 20 حالة في الربع الأول إلى 145 حالة في الربع الرابع. أما في عام 2024 فقد ارتفعت من 25 حالة في الربع الأول إلى 153 حالة في الربع الرابع.
أظهرت نتائج دراستنا أن التعرض للبعوض ووجود المياه الراكدة كانا من العوامل البيئية المرتبطة بشكل كبير بالإصابة (القيمة الاحتمالية 0.000 و0.003 على التوالي). حيث كانت نسبة التعرض للبعوض أعلى بين الحالات المؤكدة (50.8٪) مقارنة بالحالات المحتملة (35.4٪)، وكذلك وجود المياه الراكدة بنسبة (25.5٪) للحالات المؤكدة مقابل (16.2٪) للحالات المحتملة. بينما لم تُظهر عوامل مثل السفر خلال 14 يومًا أو مكان السفر أي دلائل إحصائية معتبرة.
فيما يخص تقييم المعرفة، عبّر معظم الحالات المؤكدة (89.9٪) عن معرفتهم بعوامل الخطورة التي تؤدي إلى تكاثر البعوض وكانت العوامل المتعلقة بتجمع المياه الراكدة هي الأكثر ذكرًا (79.4٪). وأفاد أغلبهم (85.8٪) بأنهم يستخدمون منتجات طاردة للبعوض. وعند سؤال الحالات المؤكدة عن الأمراض التي ينقلها البعوض ذكر (43.8٪) فيروس حمى الضنك و(19.8٪) ذكروا الملاريا.
تؤكد نتائج دراستنا أن الذكور البالغين خاصة غير السعوديين المقيمين في شمال مدينة الرياض هم الأكثر عرضة للإصابة لا سيما في الربع الأخير من السنة. وتشكل المياه الراكدة والتعرض للبعوض عوامل رئيسية في انتقال المرض وعليه يجب توجيه العوامل الوقائية نحو الفئات الأكثر خطورة مع تكثيف إجراءات مكافحة النواقل قبل وأثناء الربع الرابع من كل عام.