Article Info
Year: 2026
Month: June
Issue: 1
Pages:
Dengue Fever is the most important, rapidly spreading, emerging/re-emerging, mosquito-borne viral infection that threatens global human health and economic development.[1] According to the World Health Organization (WHO), 390 million dengue virus infections occur globally per year.[1] The incidence of dengue has grown dramatically around the world in recent decades, with cases reported to the WHO increasing from 505,430 cases in 2000 to 5.2 million in 2019.[1] Oman was considered free of dengue fever.[3,4] Although Aedes. Aegypti is well established in the south of Oman, but no local transmission of dengue fever was previously reported.[3,4] However, an outbreak of dengue fever was reported in Muscat Governorate from December 2018 to January 2019, with no travel history of the index case.[4] On 22 May 2022, the health authorities detected the first re-emergent case of dengue fever in Muscat Governorate.[4,5]
Establishing a multi-sectoral approach to control the outbreak is essential to prevent future similar outbreaks. This study described the locally transmitted dengue fever outbreak that occurred in Wilayat Nizwa, Al Dakhiliyah Governorate, Oman, from May 2023 to March 2024 and assessed the severity and the extent of the current outbreak. In addition, it described the multi-sectoral approach used to control the outbreak to prevent future similar outbreaks.
We conducted a case series study for all laboratory-confirmed dengue fever cases in Wilayat Nizwa from May 2023 to March 2024 from the Directorate General for Disease Surveillance & Control in Al-Dakhiliyah governorate. We collected data from Oman (MOH) questionnaire, an electronic e-notification system, active surveillance, and contact investigations. In Oman dengue fever case defined as “fever (temperature >38°C) lasting for 2–7 days and one or more of the following symptoms: headache, back pain, retro-orbital pain, myalgia, arthralgia, rash and hemorrhagic manifestations, with one positive test of the following; RT-PCR, Ns1, IgM.
Our study found that the total number of reported suspected and probable cases of dengue fever from May to March in Wilayat Nizwa was 547. Of these, 163 were confirmed cases of dengue fever (attack rate 121 per 100,000 population). Of the confirmed cases,85 cases (52%) were female and 159 (97.5%) were Omani, Table 1. Ages ranged from 6 months to 96 years, with a median age of 49 years (standard deviation 19.7 years), Table 1. Most cases were in the age group 60 years and above (30.67%, n = 50). Table 1.
Hospitalization was required for 35 cases (21.5%); of these, 34 (97%) cases were admitted in the general ward, while one case (3%) was admitted in the ICU. Table 1. The two most prevalent complications were increased risk of bleeding (platelet count < 50 000/ mm3; 20%; n = 7) and hepatic impairment (3%; n = 1). Table 1. All admitted cases recovered, except one death was reported in this outbreak (case fatality rate 0.6%), Table 1. Regarding the risk factors towards dengue fever, all had no recent travel history except one case, had returned from Kingdom of Saudi Arabia .6.7 % of cases had history of contact with dengue fever case at home, 24.2% observed presence of mosquito at home, 42% had history of mosquito bite and 14 % of cases were using repellent, Table 1.
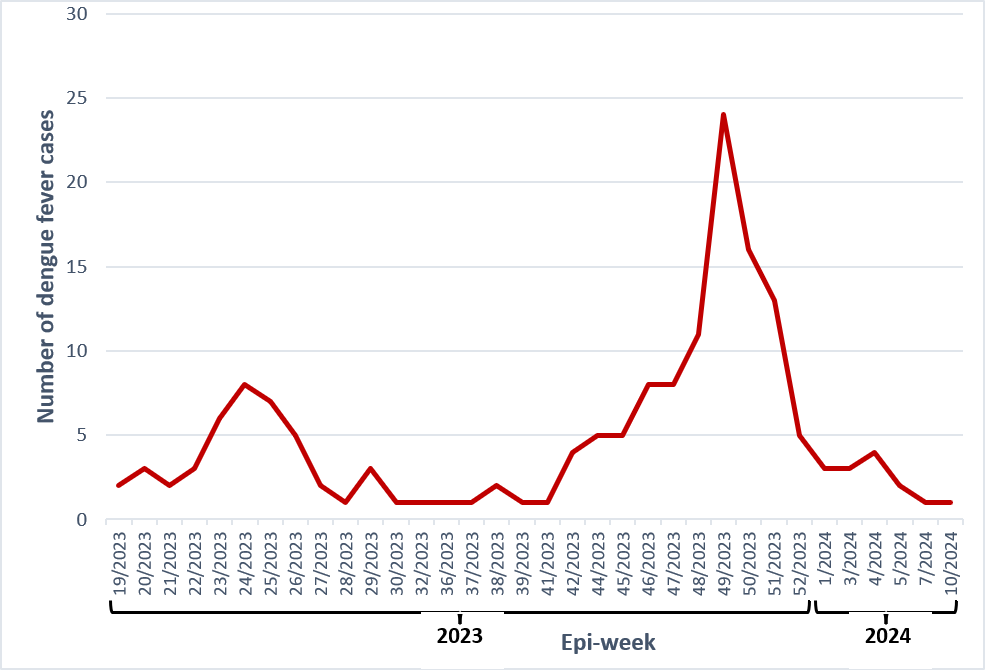
The epidemiologic curve is shown in Figure 1. There were 2 peaks on this outbreak, the first one started at epi-week 21(2023), reached the maximum at epi-week 24(2023), then declined gradually. The second peak, which was more than the first one was started in epi-week 41 (2023), reached the maximum at epi-week 49(2023), and then declined gradually, reaching the minimum on epi-week 10 (2024).
In the environmental investigation, there were pools of stagnant water and proliferation of heavy A. aegypti mosquitoes in adult, pupal, and larval forms in the affected area.
The hot and dry climate with moderate levels of rainfall in some regions of Wilayat Nizwa, in addition to behavioral factors such as water storage, may facilitate the endemicity of dengue fever in the future if proper control measures are not sustained.
In this outbreak, the overall attack rate was 121 per 100,000 population, which is higher than the first outbreak of dengue fever in Muscat. which might be due to the poor implementation of prevention and control strategies in the study area.[2,5]
Most affected cases were Female (52%), which is opposite to the first and second dengue fever outbreaks in Muscat Governorate.[2,5] This observation might be related to 44% of cases were housewives, and being exposed to mosquitoes more often in households during their daily activities, or being conscious of self-reporting. Age group 60 years and above was the highest group of reported cases, which was different than the first and second dengue fever outbreaks in Muscat Governorate and this might be related to their outdoor activities, as they have farms and animals, which are a good place for stagnant water areas.[2,5]
In this outbreak, the hospitalization rate and Hemorrhagic manifestations were less than in previous outbreaks.[2,5] All hospitalized patients with dengue fever had good outcomes except for one death. This might be attributable to early hospital admission and prompt care at an early stage of the illness. One death was reported in this outbreak (case fatality rate 0.6%), for an old man aged 90 years, a case of diabetes, who developed Dengue Shock Syndrome and hepatic impairment. In contrast, there were no reported deaths in previous outbreaks.[2,5] A multi-sectoral approach was used to control this outbreak, where teams from the Ministry of Health, Nizwa municipality, and civil society collaborated. Residents were advised to change the water in water tanks, fountains, and swimming pools every 5 days; dispose of water collected from air conditioners; dispose of used tires and damaged utensils; and cover various water reservoirs. In addition, the public was given awareness messages about measures to avoid mosquito bites, such as wearing long-sleeved wraps, using mosquito repellent on exposed body parts, using bed nets, and spraying household pesticides. A community-wide, house-to-house vector control campaign successfully terminated the outbreak
Despite all vector control measures implemented by health authorities, the elimination of A. aegypti remains challenging. Therefore, Vector surveillance should be established as a routine public health service, with enhanced surveillance, targeted vector management, and community engagement to limit dengue fever transmission.
References:
1. World Health Organization (WHO). Dengue and severe dengue [Internet]. 2024 [cited 2024 Aug 13]. Available from: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-deng….
2. Al-Abri SS, Kurup PJ, Al Manji A, Al Kindi H, Al Wahaibi A, Al Jardani A, et al. Control of the 2018–2019 dengue fever outbreak in Oman: A country previously without local transmission. International Journal of Infectious Diseases. 2020 Jan 1;90:97–103.
3. Al Awaidy ST, Khamis F. Dengue fever: An emerging disease in Oman requiring urgent public health interventions. Vol. 34, Oman Medical Journal. Oman Medical Specialty Board; 2019. p. 91–3.
4. Al Awaidy ST, Khamis F, Al-Zakwani I, Al Kindi S, Al Busafi S, Al Sulaimi K, et al. Epidemiological and Clinical Characteristics of Patients with Dengue Fever in a Recent Outbreak in Oman: A Single Center Retrospective-cohort Study. Oman Med J. 2022;37(6).
5. Al Balushi L, Al Kalbani M, Al Manji A, Amin M, Al Balushi Z, Al Barwani N, et al. A second local dengue fever outbreak: A field experience from Muscat Governorate in Oman, 2022. IJID Regions. 2023 Jun 1;7:237–41.
| Variables |
Number |
Percentage |
| Age (years) |
Mean 49 |
|
|
SD ± 19.7 |
|
|
|
Median 51 |
|
|
|
Minimum 6 months |
|
|
|
Maximum 96 years |
|
|
| Sex |
|
|
| Female |
85 |
52 |
| Male |
78 |
48 |
| Nationality |
|
|
| Omani |
159 |
97.5 |
| Non-Omani |
4 |
2.5 |
| Age group (years) |
|
|
| 0-14 |
3 |
1.84 |
| 15-29 |
34 |
20.86 |
| 30-44 |
29 |
17.79 |
| 45-59 |
47 |
28.83 |
| 60 and above |
50 |
30.67 |
| Admitted ward; |
|
|
| General ward |
34 |
97 |
| ICU |
1 |
3 |
| Complications |
|
|
| Platelet count < 50,000/mm 3 |
7 |
20 |
| Hepatic impairment |
1 |
3 |
| Outcome |
|
|
| Recovery |
34 |
97 |
| Died |
1 |
3 |
| Risk Factors |
|
|
| History of contact with sick person |
11 |
6.7 |
| History of Mosquito bite |
69 |
42.3 |
| Presence of Mosquito at home |
40 |
24.5 |
| Presence of Mosquito at work |
1 |
0.6 |
| Recent travel history |
1 |
0.6 |
| Use of repellent |
23 |
14 |
Table 1. Demographic features, complications, risk factors and outcome of dengue fever cases in Wilayat Nizwa, May 2023–March 2024
Figure 1. Epidemic curve of outbreak of dengue fever in Wilayat Nizwa, May 2023–March 2024
التقصي الوبائي لتفشي حمى الضنك في ولاية نزوى، سلطنة عمان، مايو 2023-مارس 2024
تعد حمى الضنك من أكثر الأمراض الفيروسية انتشارا بالعالم والتي تهدد الصحة والتنمية الاقتصادية. وفقا لمنظمة الصحة العالمية، فان 390 مليون إصابة بفيروس حمى الضنك سنويا. وقد زاد معدل الإصابة بحمى الضنك عالميا، حيث ارتفعت الحالات المبلغ عنها لمنظمة الصحة العالمية من 505,430 حالة في عام 2000 الى2.5 مليون عام في عام 2019. كانت عمان خالية من حمى الضنك وعلى الرغم من توطن البعوضة الزاعجة في جنوب عمان، الا أنه لم يتم التبليغ مسبقا عن انتقال محلي لحمى الضنك. في ديسمبر 2018 أبلغ عن تفشي محلي لحمى الضنك في محافظة مسقط وفي مايو 2022 تم التبليغ عن تفشي اخر لحمى الضنك.
أجريت دراسة حالة لجميع حالات حمى الضنك المؤكدة مخبريا في ولاية نزوى، من مايو 2023-مارس 2024 , تم جمع البيانات باستخدام استبيان وزارة الصحة لحمى الضنك وبرنامج الترصد الوبائي، اضافة الى البحث النشط للحالات وفحص المخالطين.
أظهرت الدراسة أن إجمالي عدد الحالات المُبلغ عنها والمُشتبه بها والمُحتملة للإصابة بحمى الضنك من مايو إلى مارس في ولاية نزوى بلغ 547 حالة. من بين هذه الحالات، كانت 163 حالة مؤكدة (معدل الإصابة 121 لكل 100,000 نسمة). من بين الحالات المُؤكدة، كانت 85 حالة (52%) من الإناث و159 حالة (97.5%) من العمانيين. تراوحت الأعمار بين 6 أشهر و96 عامًا، بمتوسط عمر 49 عامًا (الانحراف المعياري 19.7 عامًا). كانت معظم الحالات في الفئة العمرية 60 عامًا فأكثر (30.67%، عدد الحالات = 50).
تطلب دخول المستشفى 35 حالة (21.5٪)؛ من بين هؤلاء، تم إدخال 34 حالة (97٪) إلى الجناح العام، بينما تم إدخال حالة واحدة (3٪) إلى وحدة العناية المركزة. كانت المضاعفات الأكثر انتشارًا هي زيادة خطر النزيف واختلال وظائف الكبد، تعافت جميع الحالات المصابة، باستثناء حالة وفاة واحدة تم الإبلاغ عنها في هذا التفشي (معدل وفيات الحالات 0.6٪). فيما يتعلق بعوامل الخطر تجاه حمى الضنك، لم يكن لدى جميع الحالات تاريخ سفر حديث باستثناء حالة واحدة،6.7٪ من الحالات كان لديهم تاريخ مخالطة بحالة حمى الضنك في المنزل، ولاحظ 24.2٪ وجود البعوض في المنزل، وكان لدى 42٪ من الحالات لدغات البعوض وكان 14٪ من الحالات يستخدمون طاردًا للحشرات.
شهد هذا التفشي ذروتين، الأولى بدأت في الأسبوع الحادي والعشرين من الوباء (2023)، وبلغت ذروتها في الأسبوع الرابع والعشرين (2023)، ثم تراجعت تدريجيًا. أما الذروة الثانية، والتي كانت أعلى من الأولى، فقد بدأت في الأسبوع الحادي والأربعين (2023)، وبلغت ذروتها في الأسبوع التاسع والأربعين (2023)، ثم تراجعت تدريجيًا، لتصل إلى أدنى مستوى لها في الأسبوع العاشر (2024).
في الدراسة البيئية، لوحظت تجمعات من المياه الراكدة وانتشار كثيف لبعوض الزاعجة المصرية (A. aegypti) في أشكال بالغة وعذراء ويرقات في المنطقة المتأثرة.
تم القضاء على تفشي المرض بنجاح من خلال حملة مجتمعية شاملة لمكافحة النواقل. لذا يجب ارساء نظام مراقبة النواقل كخدمة صحية عامة وتعزيز الرقابة وادارة النواقل بشكل مستهدف، واشراك المجتمع للحد من انتقال حمى الضنك.